Alabama 369 Template
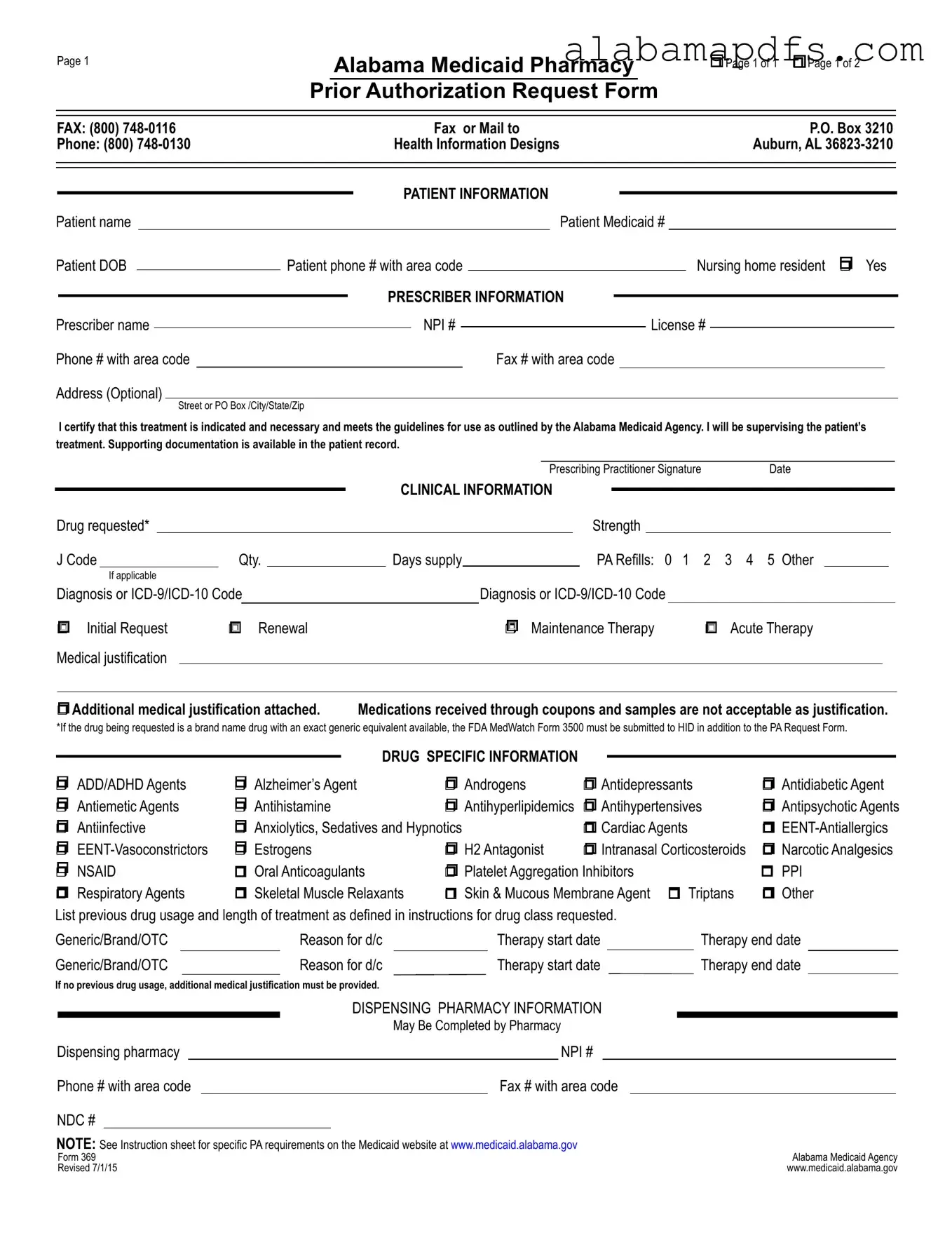
Understanding the Alabama 369 Medicaid Pharmacy Prior Authorization Request Form is crucial for healthcare providers and pharmacists who play a vital role in the healthcare of patients relying on Medicaid in Alabama. This comprehensive document is designed to facilitate the authorization process for prescription medications, ensuring that patients receive the necessary drugs while adhering to the guidelines set by the Alabama Medicaid Agency. It serves as a bridge between healthcare providers, pharmacies, and Medicaid services, streamlining patient care by requiring detailed information about the patient, the prescribing practitioner, and clinical justification for the requested medication. The form covers a wide array of drugs and specific indications, including renewal requests, maintenance therapy, and acute therapy, and it even requires detailing previous drug use and reasons for discontinuation. Additionally, it has sections for dispensing pharmacy information and specific instructions for various drug categories, highlighting its role in the efficient management of patient treatment plans and medication coverage under the Alabama Medicaid Program.
Alabama 369 Example

Page 1
Alabama Medicaid Pharmacy
Prior Authorization Request Form
rPage 1 of 1 r Page 1 of 2
FAX: (800) |
|
|
|
Fax or Mail to |
|
|
|
|
P.O. Box 3210 |
|
|||||||||||||
Phone: (800) |
|
|
Health Information Designs |
|
|
|
|
Auburn, AL |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Patient name |
|
|
|
|
|
|
|
|
Patient Medicaid # |
|
|
||||||||||||
Patient DOB |
|
|
Patient phone # with area code |
|
|
|
|
Nursing home resident r Yes |
|
||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
PRESCRIBER INFORMATION |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Prescriber name |
|
|
|
|
|
|
NPI # |
|
|
|
|
License # |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Phone # with area code |
|
|
|
|
|
|
Fax # with area code |
|
|
|
|
|
|
|
|
||||||||
Address (Optional) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
I certify that this treatment is indicated and necessary and meets the guidelines for use as outlined by the Alabama Medicaid Agency. I will be supervising the patient’s treatment. Supporting documentation is available in the patient record.
|
|
|
|
|
|
|
|
|
|
|
|
|
Prescribing Practitioner Signature |
Date |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CLINICAL INFORMATION |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Drug requested* |
|
|
|
|
|
|
|
|
|
|
|
Strength |
|
|
|
|
|
|
|
||||
|
J Code |
Qty. |
|
Days supply |
|
|
|
PA Refills: 0 1 |
2 3 4 5 Other |
|
||||||||||||||
|
|
If applicable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Diagnosis or |
|
|
|
Diagnosis or |
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
r Initial Request |
r Renewal |
|
|
|
r |
Maintenance Therapy |
r Acute Therapy |
|
|||||||||||||||
|
Medical justification |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
r Additional medical justification attached. |
Medications received through coupons and samples are not acceptable as justification. |
|
|||||||||||||||||||||
*If the drug being requested is a brand name drug with an exact generic equivalent available, the FDA MedWatch Form 3500 must be submitted to HID in addition to the PA Request Form.
|
|
|
|
|
|
|
|
|
|
DRUG SPECIFIC INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
||
r ADD/ADHD Agents |
r Alzheimer’s Agent |
r Androgens |
r Antidepressants |
r Antidiabetic Agent |
|||
r Antiemetic Agents |
r Antihistamine |
r Antihyperlipidemics |
r Antihypertensives |
r Antipsychotic Agents |
|||
r Antiinfective |
r Anxiolytics, Sedatives and Hypnotics |
r Cardiac Agents |
r |
||||
r |
r Estrogens |
r H2 Antagonist |
r Intranasal Corticosteroids |
r Narcotic Analgesics |
|||
r NSAID |
r Oral Anticoagulants |
r Platelet Aggregation Inhibitors |
r PPI |
||||
r Respiratory Agents |
r Skeletal Muscle Relaxants |
r Skin & Mucous Membrane Agent r Triptans |
r Other |
||||
List previous drug usage and length of treatment as defined in instructions for drug class requested. |
|
|
|
|
||||||||||||||
Generic/Brand/OTC |
|
Reason for d/c |
|
Therapy start date |
|
|
Therapy end date |
|
||||||||||
Generic/Brand/OTC |
|
Reason for d/c |
|
Therapy start date |
|
Therapy end date |
|
|||||||||||
If no previous drug usage, additional medical justification must be provided. |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DISPENSING PHARMACY INFORMATION |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
May Be Completed by Pharmacy |
|
|
|
|
|||||
Dispensing pharmacy |
|
|
|
|
|
NPI # |
|
|
|
|
|
|||||||
Phone # with area code |
|
|
|
|
Fax # with area code |
|
|
|
|
|
||||||||
NDC # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
NOTE: See Instruction sheet for specific PA requirements on the Medicaid website at www.medicaid.alabama.gov |
|
Alabama Medicaid Agency |
||||||||||||||||
Form 369 |
|
|
|
|
|
|
|
|
|
|||||||||
Revised 7/1/15 |
|
|
|
|
|
|
|
|
|
www.medicaid.alabama.gov |
||||||||
Page 2 |
Patient Medicaid # |
rSustained Release Oral Opioid Agonist
Proposed duration of therapy |
|
|
|
|
Is medicine for PRN use? |
r Yes |
r No |
|
|||
Type of pain r Acute r Chronic |
|
|
|
Severity of pain: r Mild |
r Moderate r Severe |
|
|||||
Is there a history of substance abuse or addiction? r Yes |
r No |
|
|
|
|||||||
If yes, is treatment plan attached? |
r Yes r No |
|
|
|
|
|
|
|
|
||
Indicate prior and/or current analgesic therapy and alternative management choices |
|
|
|
||||||||
Drug/therapy |
|
|
|
|
Reason for d/c |
|
|
|
|
|
|
Drug/therapy |
|
|
|
Reason for d/c |
|
|
|
|
|||
|
|
|
|
|
|||||||
r Antipsychotic Agents |
The request is for: |
r Monotherapy or r Polytherapy |
|
|
|||||||
For children < 6 years of age, have monitoring protocols (see Attachment C on the Alabama Medicaid website) been followed? r Yes r No For polytherapy and/or
Medical justification may include peer reviewed literature, medical record documentation, chart notes with specific symptoms that the support the diagnosis, etc.
rXenicalR
r |
If initial request |
Weight |
|
kg. |
|
Height |
|
inches |
BMI |
|
|
kg/m2 |
|||
r |
If renewal request |
Previous weight |
|
|
|
kg. |
Current weight |
|
|
|
kg. |
|
|
||
Documentation MD supervised exercise/diet regimen > 6 mo.? r Yes |
r No |
Planned adjunctive therapy? r Yes |
r No |
||||||||||||
r Phosphodiesterase Inhibitors |
|
|
|
|
|
|
|
|
||
Failure or inadequate response to the following alternate therapies: |
|
|
|
|
|
|||||
1. |
|
|
|
2. |
|
|
3. |
|
|
|
4. |
|
|
|
5. |
|
|
6. |
|
|
|
Contraindication of alternate therapies: |
|
|
|
|
|
|
|
|
||
r Documentation of vasoreactivity test attached |
r Consultation with specialist attached |
|
|
|||||||
|
|
|
|
|
|
|||||
r Specialized Nutritionals |
Height |
inches |
Current weight |
kg. |
|
|||||
rIf < 21 years of age, record supports that > 50% of need is met by specialized nutrition
rIf > 21 years of age, record supports 100% of need is met by specialized nutrition
Method of administration |
|
Duration |
|
|
|
|
# of refills |
|||
|
|
|
|
|
|
|
|
|
|
|
r Xolair® |
Current Weight:__________kg (patient’s weight must be between |
|||||||||
Is the patient 12 years or older? |
|
|
|
r |
Yes |
r |
No |
|||
Is the request for chronic idiopathic urticaria? |
r |
Yes |
r |
No |
||||||
Is the request for moderate to severe asthma and is treatment recommended by a board |
|
|
|
|
|
|
|
|||
certified pulmonologist or allergist after their evaluation (if yes answers questions below)? |
r |
Yes |
r |
No |
||||||
Has the patient had a positive skin or blood test reaction to a perennial aeroallergen? |
r |
Yes |
r |
No |
||||||
Is the patient symptomatic despite receiving a combination of either inhaled corticosteroid |
|
|
|
|
|
|
|
|||
and a leukotriene inhibitor or an inhaled corticosteroid and long acting beta agonist or has |
|
|
|
|
|
|
|
|||
the patient required 3 or more bursts of oral steroids within the past 12 months? |
r |
Yes |
r |
No |
||||||
Are the patient’s baseline IgE levels between 30 IU/mL and 700 IU/mL? |
r |
Yes |
r |
No |
||||||
Level:_________________ |
Date:__________________ |
|
|
|
|
|
|
|
||
Form 369 |
Alabama Medicaid Agency |
Revised |
www.medicaid.alabama.gov |
Form Specs
| Fact Name | Description |
|---|---|
| Form Identifier | The document is known as the "Alabama Medicaid Pharmacy Prior Authorization Request Form", commonly referred to by its form number, 369. |
| Governing Law | This form is regulated by the Alabama Medicaid Agency, under the authority of Alabama state laws governing Medicaid and pharmacy benefits. |
| Purpose | The form serves the purpose of requesting prior authorization for pharmacy medications under Medicaid. It is mandatory for certain prescriptions to ensure they are covered. |
| Submission Details | Completed forms are to be faxed or mailed to Health Information Designs in Auburn, AL, with the specific fax number and address provided on the form for submission. |
| Components of the Form | It includes sections for patient information, prescriber information, clinical information regarding the drug requested, and dispensing pharmacy details, alongside considerations for medical justification and treatment supervision. |
Detailed Guide for Writing Alabama 369
Filling out the Alabama 369 form is a process that requires attention to detail and correct information. This guide will help you through the steps needed to complete the form accurately. After completion, the form must be faxed or mailed to the appropriate contact details provided in the form. This is an essential part of ensuring that pharmacy prior authorization requests are processed smoothly and efficiently.
- Start with the Patient Information section. Fill in the patient's name, Medicaid number, date of birth (DOB), and phone number with area code. Indicate if the patient is a resident of a nursing home by marking "Yes" if applicable.
- Move on to the Prescriber Information section. Enter the prescriber's name, their National Provider Identifier (NPI) number, license number, phone and fax numbers with area codes, and address if available. The prescriber needs to sign and date the form, certifying that the treatment is necessary and meets Alabama Medicaid's guidelines.
- In the Clinical Information area, specify the drug requested, its strength, J Code (if applicable), quantity, days' supply, and the number of refills required. If relevant, provide the diagnosis or ICD-9/ICD-10 Code. Check the appropriate boxes to indicate if this is an initial request, renewal, maintenance therapy, or acute therapy and if additional medical justification is attached.
- Detail any previous drug usage, including the name of the drug (generic/brand/OTC), reason for discontinuation, start and end dates of therapy. If there was no previous drug usage, mention that additional medical justification will be provided.
- Under Drug Specific Information, select the category that the requested drug falls into and list any previous medications as instructed in the form.
- Fill in the Dispensing Pharmacy Information section with the pharmacy's NPI number, phone and fax numbers with area codes, and the NDC number of the requested medication.
- If applicable to your request, complete the additional sections that pertains to specific medication requests or conditions, such as details about opioid use, analgesic therapy history, or requirements for special medications like Xolair®.
After you've filled out the form, make sure all the information is correct and complete. Missing or incorrect information can delay the process. Once everything is in order, fax or mail the form to the contact details provided. This will initiate the review process, which is essential for obtaining the necessary authorization for medication under the Alabama Medicaid program. Remember to keep a copy of the form for your records.
Common Questions
What is the Alabama 369 form used for?
The Alabama 369 form is utilized to request prior authorization for specific pharmacy prescriptions under the Alabama Medicaid program. This process ensures that the requested medication is covered and meets the criteria set forth by the Alabama Medicaid Agency, ensuring it is indicated, necessary, and appropriate for the patient's treatment plan.
How can the form be submitted?
The completed form can be submitted either by fax or mail. For fax submissions, the number is (800) 748-0116. If choosing to mail the form, it should be sent to P.O. Box 3210, Auburn, AL 36823-3210. This provides flexibility in how prescribers can submit their requests for authorization.
Who needs to complete the Alabama 369 form?
This form must be completed by the prescribing practitioner who is overseeing the patient's treatment. It requires the prescriber's certification that the requested medication is necessary for the patient's treatment and that it aligns with the guidelines provided by the Alabama Medicaid Agency.
What information is required on the form?
Essential details such as patient information (including Medicaid number and date of birth), prescriber information (including NPI and license numbers), clinical information regarding the requested medication, and any relevant diagnosis codes. Additionally, the prescribing practitioner must sign the form to certify the treatment's necessity.
Is supporting documentation required?
Yes, the prescriber must indicate if additional medical justification is attached. This documentation supports the request and can include peer-reviewed literature, medical record documentation, and specific symptoms that justify the diagnosis and treatment plan.
Can medications received through coupons and samples be used as justification?
No, medications that have been received through coupons or as samples are not acceptable forms of justification for a prior authorization request according to the instructions on the form.
What should be done if the drug requested has a generic equivalent?
If the requested medication is a brand name drug that has an available generic equivalent, the FDA MedWatch Form 3500 must be submitted in addition to the Prior Authorization Request Form. This requirement ensures that the necessity for the brand name drug over the generic is adequately documented and justified.
How is information regarding previous drug usage included?
The form allows for detailing previous medications the patient has been prescribed, the reason for discontinuation, and the start and end dates of each therapy. This information helps in understanding the patient's medication history and the rationale behind the current medication request.
Who completes the section on dispensing pharmacy information?
This section may be completed by the pharmacy that will be dispensing the medication. It requires the pharmacy's NPI number, contact information, and the National Drug Code (NDC) for the requested medication, facilitating the dispensing process once the authorization is granted.
Where can instructions for completing the form be found?
Instructions for specific Prior Authorization requirements can be found on the Alabama Medicaid website at www.medicaid.alabama.gov. This resource provides additional guidance on how to properly fill out and submit the form, ensuring that all necessary information is accurately provided.
Common mistakes
Filling out the Alabama Medicaid Pharmacy Prior Authorization Request Form, commonly known as Form 369, is a crucial step in ensuring that patients receive the medications they need. However, this task can be daunting, and mistakes are often made. Understanding these errors can improve the process, making it smoother for both healthcare providers and patients.
Incorrect Patient Information: One common error is the incorrect entry of patient details. This includes spelling mistakes in the patient’s name, wrong Medicaid numbers, or incorrect dates of birth. These inaccuracies can lead to delays or outright denials of medication coverage because the information does not match Medicaid records.
Failing to Specify Drug Details: Another frequent mistake is not providing complete details about the drug requested. This entails overlooking to fill in the drug strength, quantity, number of days' supply, and the exact medication name. Given that some medications have multiple strengths or forms, omitting these details can lead to confusion or incorrect medication dispensing.
Omitting Clinical Information: The clinical rationale for the requested medication is vital. Neglecting to include a diagnosis or ICD-10 code, forgetting to state whether the request is for initial therapy or a renewal, and not providing supporting clinical information or medical justification are critical oversights. Without this, reviewers won't understand the medical necessity behind the prescription, potentially resulting in a denial.
Skipping Prescriber Credentials: Healthcare providers sometimes forget to include their National Provider Identifier (NPI) number, state license number, and contact information. This oversight makes it impossible for the form reviewers to verify the prescriber's authority to request the medication, which is crucial for form approval.
Overlooking Signature and Date: The most straightforward yet often forgotten part is the prescriber’s signature and the date. Without this, the form is considered incomplete and cannot be processed. The signature certifies the prescriber's validation that the treatment is necessary and has been indicated following Alabama Medicaid's guidelines.
To avoid these common errors, double-checking the form before submission is essential. Ensuring attentiveness to detail can significantly ease the prior authorization process, facilitating quicker access to necessary medications for patients. By doing so, healthcare providers support the goal of delivering timely and appropriate care, ultimately fostering better health outcomes for individuals under their care.
Documents used along the form
When processing the Alabama Medicaid Pharmacy Prior Authorization Request, commonly recognized as the Alabama 369 form, healthcare providers are often required to include additional forms and documentation to ensure a comprehensive review and approval process. These documents play a crucial role in providing detailed patient information, medical justification for the prescribed medication, and compliance with Alabama Medicaid policies.
- Medication History Form: This document catalogs all medications a patient has taken previously, including over-the-counter drugs, prescriptions, and samples. It helps in evaluating the patient’s response to various treatments and identifying any patterns of drug interaction or side effects.
- Physician Certification Statement (PCS): The PCS is a declaration by the treating physician that the prescribed medication is necessary for the patient’s treatment plan. It often includes details about the diagnosis, prognosis, and expected benefits of the medication.
- FDA MedWatch Form 3500: For prescription medications that have caused adverse reactions in a patient, this form is used to report the incident to the FDA. It’s particularly important when requesting authorization for drugs with known side effects or when switching from a generic to a brand-name drug due to intolerance.
- Specialist Consultation Report: If the patient has been referred to a specialist for their condition, the specialist's findings and recommendations are crucial. This report provides a detailed analysis of the patient’s condition from a specialist’s perspective and offers justification for the chosen treatment.
- Medical Record Documentation: Comprehensive medical records, including chart notes, lab results, and diagnostic reports, provide a detailed medical history of the patient. This documentation supports the medical necessity of the medication request.
- Treatment Plan: A detailed treatment plan outlines the objectives, strategies, and expected outcomes of the prescribed medication. It may also include information on monitoring and follow-up plans to evaluate the effectiveness of the medication.
Together, these documents contribute to a well-supported Prior Authorization request by offering a holistic view of the patient’s medical history and current health status. It’s essential for healthcare providers to compile these documents meticulously to facilitate a smooth review process by the Alabama Medicaid Agency, ensuring that patients receive the medications they need promptly and efficiently.
Similar forms
The Alabama 369 form, designed for Alabama Medicaid Pharmacy Prior Authorization Request, shares similarities with several other forms used in healthcare and pharmacy management. These similarities rest in their purpose, structure, and the type of information they solicit from healthcare professionals to process requests related to patient care and medication management. However, it's crucial to understand how these forms compare to understand the Alabama 369 form's specific role within Medicaid's framework.
CMS-10114 National Prior Authorization Form
The CMS-10114 form, recognized nationwide, is utilized for prior authorization requests across various healthcare services, including pharmacy benefits but not limited to them. Like the Alabama 369 form, the CMS-10114 collects comprehensive patient and prescriber information, clinical justification for the requested service or medication, and requires a prescriber's signature to attest to the necessity of the request. Both forms aim to streamline the process of acquiring necessary approvals for patient treatment, ensuring that patients receive timely access to their medications or services. The main distinction lies in their scope, where the CMS-10114's application extends beyond pharmacy-related requests to a broader range of healthcare services.
FAA MedXPress Form 8500-8
While primarily intended for use by applicants for FAA airman medical certification, the FAA MedXPress Form 8500-8 shares a conceptual similarity with the Alabama 369 form in gathering detailed personal health information. This FAA form collects comprehensive medical history, medications, visits to health professionals, and other health-related information to assess the applicant's fitness for flying. Despite their vastly different contexts – one for flight certification and the other for Medicaid pharmacy prior authorization – both forms play critical roles in evaluating the health and safety of individuals within their respective spheres. The main similarity lies in their thorough approach to collecting health information to support decision-making, albeit for different end purposes.
FDA Form 3500
The FDA Form 3500 is intended for voluntary reporting of adverse events and product problems related to FDA-regulated products. This can include medications, which makes it relevant in a discussion about the Alabama 369 form. Both forms require detailed information about the drug in question, including the drug name, dosage, and any adverse effects observed. The key similarity lies in their commitment to patient safety and the appropriate use of medications. However, the FDA Form 3500 is focused on post-market surveillance and the collection of data on adverse events to protect public health, while the Alabama 369 form is primarily used for the pre-approval process of medication therapy under the Alabama Medicaid program.
Dos and Don'ts
When completing the Alabama Medicaid Pharmacy Prior Authorization Request Form, also known as Form 369, it's important to pay close attention to the details and requirements to ensure a smooth process. Here's a helpful list of do's and don'ts to guide you through filling out the form.
Do:- Double-check the patient's Medicaid number and date of birth (DOB) for accuracy. These are critical pieces of information that must be correct to avoid processing delays.
- Ensure the prescriber's information, including the NPI (National Provider Identifier) and license numbers, is complete and clearly written. This is vital for validating the prescriber's authority to request the medication.
- Provide detailed clinical information, including the drug requested, dosage, and medical justification. Clear and complete clinical details support the necessity of the prescription and facilitate quicker approval.
- Attach any required additional documentation, such as the FDA MedWatch Form 3500 for brand-name drugs with an exact generic equivalent or supporting medical justifications that outline the need for the specific requested medication.
- Indicate the type of therapy (initial request, renewal, maintenance therapy, or acute therapy) clearly, to help streamline the review process.
- Include a detailed medication history, especially if previous treatments have been tried and discontinued. This information is crucial for understanding the patient's background and the rationale behind the current request.
- Contact the issuing pharmacy to fill in their information if necessary, ensuring that the dispensing pharmacy’s NPI, phone, and fax numbers are correctly provided.
- Leave sections incomplete. Make sure every required field is filled out. If a section doesn't apply, indicate this with "N/A" or "None" to show that the question was not overlooked.
- Use medical jargon without explanation. Remember, not everyone who reviews these forms may have a medical background. Where medical terms are necessary, provide clear explanations or details.
- Assume that more information is not necessary. If in doubt, provide additional context or clarification. It's better to offer too much information than too little.
- Forget to update the patient and prescriber contact information, including current phone numbers with area codes. This ensures that any follow-up or clarification can be done efficiently.
- Rely on medications received through coupons and samples as justification for the medical necessity of the treatment. These are not considered valid forms of justification.
- Submit the form without the prescribing practitioner's signature and date, as these are required to authenticate and endorse the request.
- Ignore the specific PA requirements listed on the Medicaid website. Each medication or treatment may have its own set of prerequisites for approval.
By following these guidelines, you can help ensure that the Alabama Medicaid Pharmacy Prior Authorization Request Form is completed thoroughly and accurately, which can help facilitate a smoother review and approval process.
Misconceptions
Understanding the Alabama Medicaid Pharmacy Prior Authorization Request Form, commonly referred to as Form 369, is crucial for healthcare providers and patients alike. However, there are several misconceptions surrounding this form. Here, we aim to clarify these misunderstandings to help ensure that the process is as smooth as possible for everyone involved.
Only brand-name drugs require prior authorization. This is not true. While the form specifically mentions brand-name drugs with a generic equivalent, prior authorization can be required for both brand-name and generic drugs, depending on Alabama Medicaid’s formulary and guidelines.
Form 369 can be submitted for emergency medications. In reality, the prior authorization process is not designed for emergency situations. In an emergency, medications might be dispensed in accordance with pharmacy guidelines, bypasséing the need for Form 369, although this action may depend on specific circumstances and regulations.
Patients can submit Form 369 on their own. The form is intended to be completed and submitted by healthcare providers, not patients. This process ensures that all necessary clinical information and justification for the medication are accurately provided.
Any pharmacy can dispense medications approved via Form 369. While most medications approved for prior authorization can be dispensed by any participating pharmacy, certain drugs may have more restrictive dispensing requirements due to their nature or cost.
Approval is guaranteed once the form is submitted. Submission of Form 369 does not guarantee approval. The request must first be reviewed and meet Alabama Medicaid’s criteria for medical necessity and appropriateness based on the provided clinical information.
The form is only for prescription medications. While primarily used for prescription medications, Form 369 also encompasses requests for specific over-the-counter medications if deemed medically necessary and is included under the patient's benefit plan.
Form 369 is valid indefinitely once approved. Approvals for medication through Form 369 have specified durations. Upon expiration, a renewal request must be submitted for continued approval, if still medically necessary.
A single Form 369 can cover multiple medications. Generally, a separate Form 369 is required for each medication that requires prior authorization. This ensures each medication is reviewed for its specific clinical circumstances and medical necessity.
Supporting documentation is rarely needed. On the contrary, providing relevant medical justifications, documentation, and previous treatment information is crucial for the approval process. This supports the request and demonstrates compliance with Alabama Medicaid guidelines.
Coupons and samples can be used to justify medical necessity. Actually, medications received through coupons and samples are not acceptable justifications for medical necessity on Form 369. The prescriber must provide clinical evidence and history of the medication’s use and its effectiveness for the patient.
It's important for all parties involved to understand these aspects of the Alabama Medicaid Pharmacy Prior Authorization Request Form to facilitate timely access to necessary medications for Medicaid recipients. Having accurate and complete information can significantly streamline the approval process.
Key takeaways
Filling out the Alabama 369 form correctly is crucial for the timely processing of pharmacy prior authorization requests. Understanding this can streamline the process and ensure patients receive the necessary medications without unnecessary delays. Here are key takeaways to consider:
- Ensure accurate completion of patient information, including Medicaid number, date of birth (DOB), and phone number. This helps the Alabama Medicaid Agency quickly identify the patient.
- Prescriber information is critical; provide the National Provider Identifier (NPI) number, license number, and contact information to ensure the request can be verified and followed up on if necessary.
- For the requested drug, include specifics such as strength, quantity, days supply, and any refills. This clarity prevents any confusion and speeds up the authorization process.
- The clinical information section should be filled out meticulously, indicating whether the request is an initial one, a renewal, maintenance, or acute therapy. This aids in the understanding of the patient's medical need.
- If the medication requested has a generic equivalent, ensure to submit an FDA MedWatch Form 3500 alongside the PA Request Form as required.
- Detailing previous drug usage including the reasons for discontinuation, therapy start, and end dates is necessary for context on the patient's past medication history and its effectiveness.
- The dispensing pharmacy’s information, including NPI and contact details, is important for where the medication will be sent once approved, facilitating the dispensation process.
- Lastly, the inclusion of a supporting document, such as the treatment plan for patients with a history of substance abuse when applicable, is crucial for a comprehensive review of the necessity and appropriateness of the medication request.
By following these guidelines and carefully reviewing all sections of the Alabama 369 form, prescribers and pharmacists can effectively work together to ensure that patients receive the medications they need in a timely manner.
Check out Popular PDFs
C 25B Alabama - It signifies the culmination of the legal eviction process, offering a formal pathway to resolving untenable tenancy situations.
Alabama Child Support Forms - A regulatory document designed to standardize the reporting of income and expenses for the calculation of child support in Alabama.